Pain-Free Movement Starts Here.
Slipped Disc Treatment in Faridabad – Advanced Spine Care for Lasting Pain Relief
Looking for the best slipped disc treatment in Faridabad? Suffering from lower back pain, sciatica, or herniated disc problems? Our advanced orthopedic and spine care center offers world-class slipped disc treatment in Faridabad, India, combining expert diagnosis, modern technology, and compassionate patient care.
We specialize in non-surgical and surgical spine treatments, helping patients regain mobility, comfort, and quality of life — safely and effectively.
📞 Book Your Consultation Today | Same-Day Appointments Available
- Expert Orthopedic Surgeon:- MBBS, MS (Orthopaedics), DNB (Orthopaedics), Fellowship in Spine Surgery
- Spine Specialist:- Specialize in Fully Endoscopic Spine Surgeries for various spine pathologies
- Experience:- 14 years of experience in treating complex spine, joint, and sports-related injuries
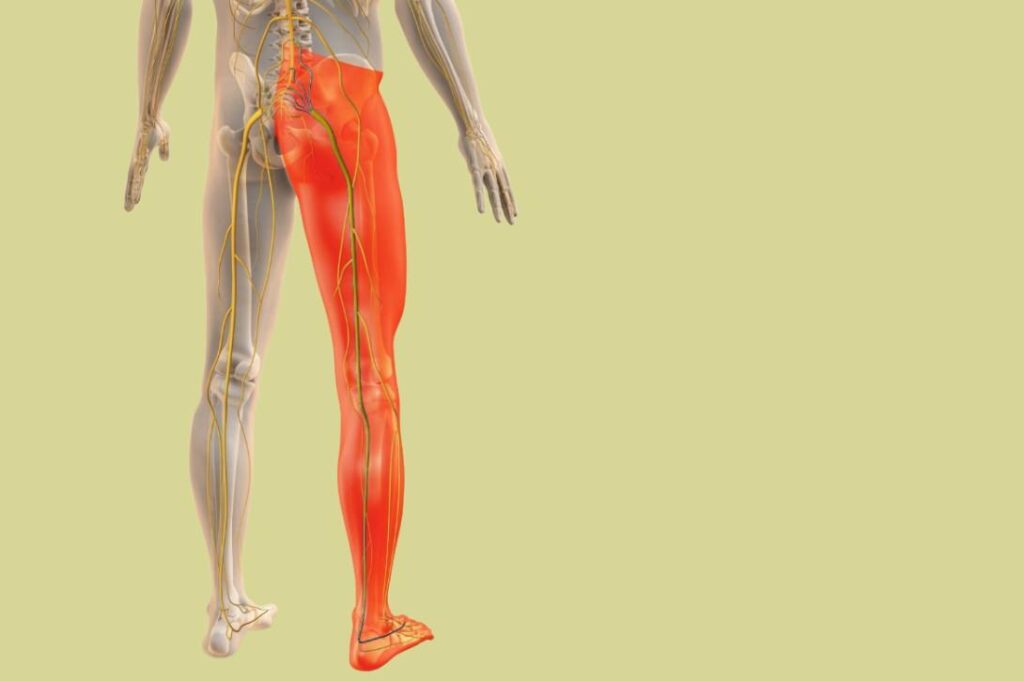
What is a Slipped Disc? (Herniated Disk Explained)

A slipped disc, also known as herniated disk or disc prolapse, occurs when the soft cushion-like disc between two spinal bones moves out of its normal position. This can irritate nearby nerves, causing pain, numbness, or weakness.
Most slipped discs do not cause symptoms, but when the disc presses against nerve roots, it leads to sciatica and severe lower back pain.
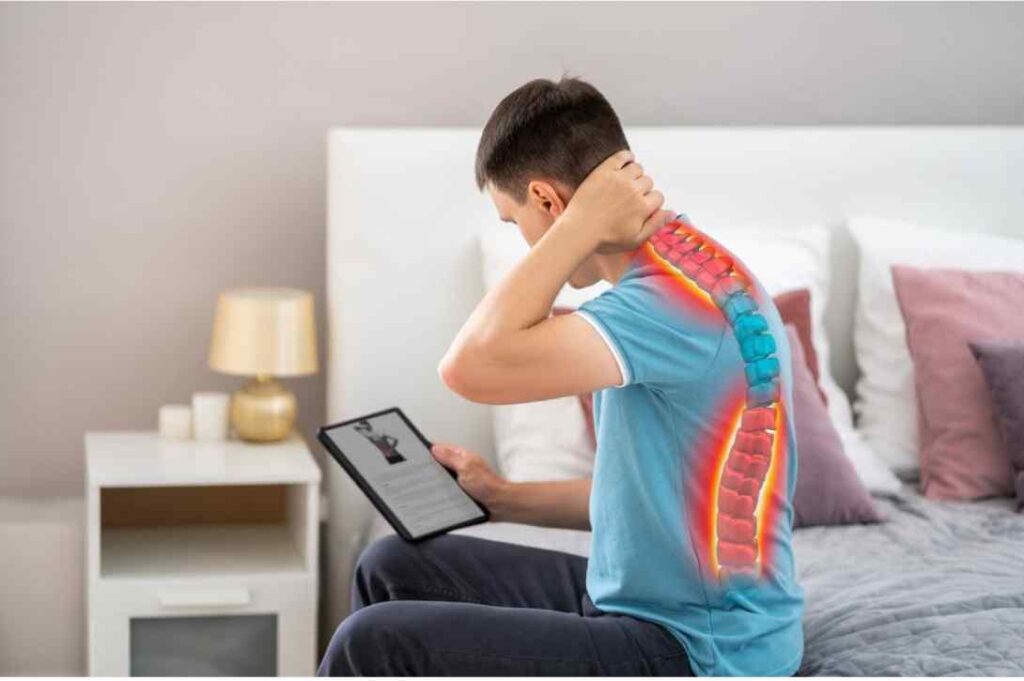
Common Symptoms of Slipped Disc Lower Back Pain:
- Radiating pain from lower back to leg & foot
- Tingling, numbness, or heaviness in legs
- Weakness in ankle or toes (foot drop / toe drop)
- Difficulty walking or standing
- In severe cases, bowel or bladder control problems
If you are experiencing these symptoms, early diagnosis and treatment can prevent long-term nerve damage.
Comprehensive Lower Back Pain Treatment in Faridabad
Our hospital offers complete lower back pain treatment in Faridabad, focusing on accurate diagnosis and customized care

HARNIATED DISK /SLIPPED DISC
CERVICAL SPONDYLOSIS
SCIATICA PAIN
DISC BULGE

CHRONIC LOWER BACK PAIN

LUMBAR SPONDYLOSIS
Advanced Spine Surgery in Faridabad – When Surgery is Needed
If non-surgical treatments fail or if neurological symptoms worsen, we offer minimally invasive spine surgery in Faridabad using the latest techniques.
Our Spine Surgery Treatments Include:
- Microdiscectomy
- Endoscopic Spine Surgery
- Minimally Invasive Spine Surgery
- Complex Spine Reconstruction
Our spine surgery treatment in Faridabad ensures:
- Smaller incisions
- Faster recovery
- Minimal blood loss
- Shorter hospital stay
- High success rates

Non-Surgical Slipped Disc Treatment Options
We provide advanced conservative management techniques for effective pain relief:

Physical Therapy & Rehabilitation
Customized physiotherapy programs focusing on:
- Core muscle strengthening
- Posture correction
- Flexibility exercises
- Pain relief therapies (TENS, IFT, hot/cold packs)
Rest & Pain Management
Short-term bed rest combined with anti-inflammatory medications to reduce acute pain and swelling.

Rest & Pain Management
Short-term bed rest combined with anti-inflammatory medications to reduce acute pain and swelling.

Lifestyle & Ergonomic Guidance
- Workplace posture correction
- Weight management
- Safe lifting techniques
- Exercise routines for long-term spine health
Lifestyle & Ergonomic Guidance
- Workplace posture correction
- Weight management
- Safe lifting techniques
- Exercise routines for long-term spine health

Spine Injections - Epidural & Nerve Root Blocks
These advanced injections reduce nerve inflammation, relieve pain, and often delay or avoid surgery.
Spine Injections - Epidural & Nerve Root Blocks
These advanced injections reduce nerve inflammation, relieve pain, and often delay or avoid surgery.

Advanced Spine Surgery in Faridabad – When Surgery is Needed
If non-surgical treatments fail or if neurological symptoms worsen, we offer minimally invasive spine surgery in Faridabad using the latest techniques.
Our Spine Surgery Treatments Include:
- Endoscopic Spine Surgery
- Microdiscectomy
- Minimally Invasive Spine Surgery
- Complex Spine Reconstruction
Our spine surgery treatment in Faridabad ensures:
- Smaller incisions
- Faster recovery
- Minimal blood loss
- Shorter hospital stay
- High success rates
Best Slip Disc Treatment Hospital Near Faridabad
Recognized as one of the best slipped disc hospitals in Faridabad, our center provides complete spine care under one roof, from diagnosis to surgery and rehabilitation.
Patients from across Faridabad, Delhi NCR, and Haryana trust us for:
- Ethical treatment
- Modern infrastructure
- Highly skilled spine specialists
- Excellent post-treatment support
Why Early Treatment Matters?
Delaying treatment can lead to:
- Permanent nerve damage
- Chronic pain
- Reduced mobility
- Long-term disability
Early diagnosis and professional treatment ensure faster healing, better outcomes, and reduced complications.
Revolutionary Technology
Cutting-edge innovation for safer spine treatment.
Revolutionary Technology
Cutting-edge innovation for safer spine treatment.
Protects Mobility
Ensures a faster recovery with no compromise on function.
Affordable & Accessible
World-class spine care at a reasonable cost.
Frequently Asked Questions
No. Only 10% of slipped disc cases require surgery.
Most patients recover with non-surgical treatments and guided rehabilitation.
Our doctors always recommend conservative treatment first, ensuring surgery is performed only when absolutely necessary.
Recovery usually takes 4 to 12 weeks with proper rest, medications, physiotherapy, and rehabilitation. Some patients may recover faster, while others with severe disc prolapse may require longer recovery or surgery.
Yes. With modern techniques like minimally invasive spine surgery, procedures are highly safe, precise, and effective, with faster recovery, minimal scarring, and lower complication rates when performed by experienced spine surgeons.
Yes, many cases heal naturally with rest, medication, and physiotherapy.
Early symptoms include:
- Persistent lower back pain
- Radiating pain to leg or foot (sciatica)
- Tingling or numbness
- Muscle weakness
- Difficulty standing, sitting, or walking
Early treatment helps prevent nerve damage and chronic pain.
The cost depends on severity, diagnostic tests, treatment type, hospital infrastructure, and whether surgery is needed. Non-surgical treatment is affordable, while spine surgery treatment in Faridabad may vary based on the technique used. For accurate estimates, consultation is recommended.
Prevention tips include:
- Regular core strengthening exercises
- Correct posture while sitting and standing
- Using ergonomic chairs at work
- Avoiding heavy lifting and forward bending
- Maintaining healthy body weight