Ankylosing Spondylitis: Early Signs, Diagnosis Tests, and the Right Treatment Plan
If you wake up every morning with a stiff lower back that loosens up after an hour of movement — do not ignore it. It could be more than just bad posture or muscle fatigue. It might be Ankylosing Spondylitis (AS), a chronic inflammatory disease of the spine that affects millions of people — and is frequently misdiagnosed for years.
What Is Ankylosing Spondylitis?
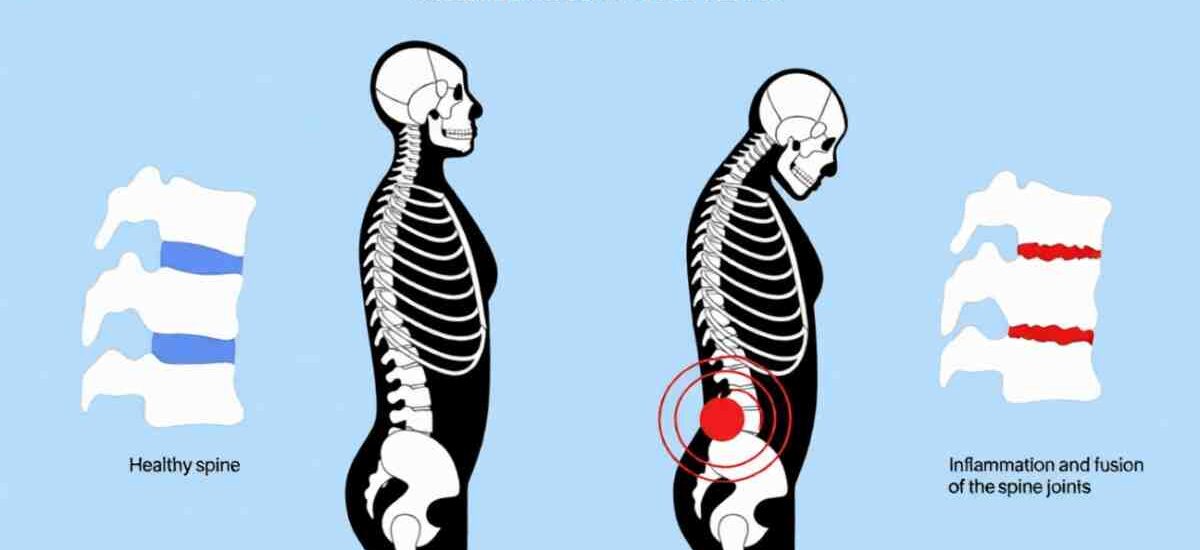
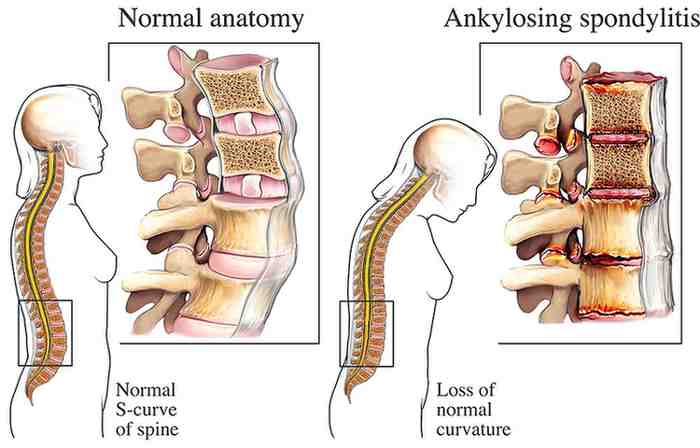
Ankylosing Spondylitis (AS) is a form of chronic inflammatory arthritis that primarily affects the spine and sacroiliac joints — the joints connecting your lower spine to your pelvis. Over time, the inflammation can cause the vertebrae of the spine to fuse together, leading to pain, progressive stiffness, and in severe cases, a stooped posture known as ‘chin-on-chest’ deformity.
What makes Ankylosing Spondylitis particularly tricky is that it is not a disease of sudden onset. It is a slow, progressive condition — which means many patients spend years bouncing between orthopedic doctors, spine surgeons, and physiotherapists without ever receiving a proper, unified treatment plan.
This is why a comprehensive, multidisciplinary approach — involving spinal surgeons, physiotherapists, Pilates trainers, yoga therapists, psychologists, and nutritionists — is the cornerstone of effective AS management.
Early Signs and Symptoms of Ankylosing Spondylitis
Recognizing Ankylosing Spondylitis early is critical to preventing long-term damage. The symptoms of AS are distinct — if you know what to look for. Here are the most important early warning signs:
1. Morning Stiffness in the Lower Back and Hips
The hallmark symptom of Ankylosing Spondylitis is morning stiffness. After a full night’s rest, the body — particularly the lower back and hips — feels intensely stiff and rigid. Patients often describe feeling unable to get out of bed easily after waking up.
The key characteristic that separates AS from ordinary back pain is this: the stiffness gradually improves within 30 minutes to an hour of movement and activity. The person functions relatively normally throughout the rest of the day, only to experience the same cycle of stiffness the next morning.
2. Pain in the Sacroiliac Region
Patients with Ankylosing Spondylitis typically report pain around the lower back — specifically about 1 to 1.5 inches on either side of the center of the spine. This is the location of the sacroiliac joints, and tenderness or pain in this area is a strong clinical indicator of AS.
Two joints are classically involved in Ankylosing Spondylitis: the sacroiliac joints and the hip joints. Involvement of either or both should raise the suspicion for AS.
3. Reduced Spinal Flexibility
As the disease progresses, the spine gradually loses its natural range of motion. This leads to a reduced ability to bend forward, sideways, or rotate the torso.
4. Fatigue and Generalized Discomfort
Because AS is an inflammatory disease, it does not just affect the joints. Patients commonly experience chronic fatigue, a general sense of feeling unwell, and reduced energy levels — all of which are systemic effects of persistent inflammation in the body.
The Schober’s Test: A Simple At-Home Check for Ankylosing Spondylitis
One of the most clinically recognized tests for spinal flexibility loss in Ankylosing Spondylitis is the Schober’s Test. Here is how you can perform a simplified version at home:
- Stand straight with both feet together and your knees fully extended — do not bend your knees.
- Slowly bend forward and try to touch your toes with the tips of your fingers.
- If you can comfortably touch your toes, your spinal flexibility is likely within normal range.
- If there is a gap of more than 5 centimeters between your fingertips and the floor — this is a significant clinical sign.
A fingertip-to-floor distance of more than 5 cm, combined with morning stiffness and sacroiliac pain, is a strong indicator that you should consult a spine specialist for further evaluation of Ankylosing Spondylitis.
How Is Ankylosing Spondylitis Diagnosed?
Ankylosing Spondylitis is fundamentally a genetic disease — but genetics alone does not determine whether you develop it. Understanding the diagnosis involves two key components: the genetic marker and the environmental trigger.
The HLA-B27 Genetic Test
The HLA-B27 test is a blood test that checks for the presence of a specific genetic marker — the Human Leukocyte Antigen B27 (HLA-B27). The vast majority of Ankylosing Spondylitis patients test positive for HLA-B27.
However, it is important to understand that a positive HLA-B27 result does not automatically mean you have AS. Many people carry this gene but never develop the disease in their lifetime. Conversely, being negative for HLA-B27 does not entirely rule out AS.
A useful way to understand this: genetics loads the gun, but the environment pulls the trigger.
What Triggers Ankylosing Spondylitis?
If you are HLA-B27 positive, the following environmental triggers can activate or worsen the disease:
- Gut infections or gastrointestinal inflammation
- Viral infections
- Chronic physical or emotional stress
Sedentary lifestyle and prolonged inactivity.
Other Diagnostic Tests for Ankylosing Spondylitis
Beyond the HLA-B27 test, doctors typically use a combination of the following to confirm diagnosis:
- MRI scan of the sacroiliac joints — to detect early inflammation before bony changes appear on X-ray
- X-ray of the pelvis and spine — to assess joint damage and fusion in advanced cases
- Blood tests for CRP and ESR — inflammatory markers that are elevated during active disease flares
- Clinical assessment — physical examination of spinal mobility, posture, and sacroiliac tenderness
The Spectrum of Ankylosing Spondylitis: From No Symptoms to Severe Deformity
One of the most important things to understand about AS is that it exists on a wide spectrum. Not every patient with Ankylosing Spondylitis will develop the dramatic spinal curvature that appears in medical textbooks. The disease ranges from:
- Asymptomatic (HLA-B27 positive with no symptoms at all)
- Mild (occasional morning stiffness, manageable with exercise and over-the-counter medication)
- Moderate (persistent pain, reduced mobility, requires physiotherapy and prescription medication)
- Severe (significant deformity, hip or back fusion, requiring surgical intervention)
The good news is that the vast majority of patients with Ankylosing Spondylitis have mild to moderate disease — which can be managed effectively without surgery, provided treatment is consistent and begins early.
Treatment of Ankylosing Spondylitis: A Comprehensive Approach
Effective Ankylosing Spondylitis treatment is not a single pill or a quick fix. It requires a multi-pronged strategy that addresses inflammation, mobility, posture, mental health, and lifestyle — simultaneously. Here is a breakdown of the key treatment pillars:

1. Physiotherapy: The Cornerstone of AS Management
Physiotherapy is the single most important non-surgical treatment for Ankylosing Spondylitis. The body’s natural tendency in AS is to progressively stiffen — and the only way to fight this is through consistent, targeted movement.
Physiotherapy for AS typically includes:
- Postural correction exercises — to counter the characteristic forward-stooped posture
- Stretching exercises — general body stretches targeting the low back, hips, and thoracic spine
- Core muscle strengthening — building a strong core to support and protect the spine
- Breathing exercises — to maintain chest and rib cage mobility, which is often compromised in AS
- Moist heat packs — to warm the joints before exercise, improving comfort and suppleness
Electrotherapy — for pain management during flare-ups
2. Pilates, Yoga, and Hydrotherapy
Any exercise that promotes full-body flexibility — particularly in the lower back and hip regions — is highly beneficial for Ankylosing Spondylitis patients. Pilates and yoga are especially recommended because they combine controlled stretching, core strengthening, and breathing — the three pillars of AS exercise management.
Swimming and hydrotherapy are equally valuable. The buoyancy of water reduces joint stress while allowing full-range movement — making it ideal for AS patients with pain or joint stiffness.
Exercise in Ankylosing Spondylitis is not optional — it is as essential as eating and breathing. It must become a permanent part of your daily lifestyle, not just a phase of treatment.
3. Medications for Ankylosing Spondylitis
Because AS is an inflammatory condition, medications focus on reducing and controlling inflammation throughout the body. The treatment regimen can span months and years, and may include:
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) — the first line of treatment for pain and inflammation
- Disease-Modifying Anti-Rheumatic Drugs (DMARDs) — for moderate to severe disease
- Biologics (TNF inhibitors, IL-17 inhibitors) — for patients who do not respond to conventional medications
Medications should always be prescribed and monitored by a qualified rheumatologist or spine specialist. Self-medication is not appropriate for a chronic inflammatory condition like AS.
4. Surgery: When Is It Required?
The vast majority of Ankylosing Spondylitis patients never need surgery. However, in a small number of cases where the disease progresses to severe joint damage, the following surgical procedures may be considered:
- Total Hip Replacement — for severe hip joint destruction (approximately 1 in 100 patients)
- Spinal Osteotomy / Deformity Correction — for extreme spinal curvature deformity (extremely rare, approximately 1 in a million patients)
If you have been diagnosed with Ankylosing Spondylitis, there is no reason to fear surgery. Consistent medical treatment and exercise significantly reduces the chances of ever reaching this stage.
5. Psychological Counseling and Mental Health Support
A diagnosis of a chronic, lifelong condition can be emotionally overwhelming. Many patients feel anxious, discouraged, or fearful after being told they have Ankylosing Spondylitis — especially when they read about worst-case outcomes online.
This is where psychological counseling plays an essential role. A problem-solving approach to chronic illness — focusing on what you can do rather than what you cannot — has been shown to significantly improve patient outcomes and quality of life.
Ankylosing Spondylitis is not curable, but it is absolutely manageable. Think of it in the same category as diabetes, hypertension, or thyroid conditions — chronic conditions that millions of people live with comfortably through proper management. People with AS can and do live full, active, healthy lives.
Living with Ankylosing Spondylitis: Lifestyle Tips for Long-Term Management
Beyond formal treatment, making the right lifestyle choices can have a significant impact on the progression and day-to-day experience of Ankylosing Spondylitis:
- Exercise every single day — even on good days. Consistency is non-negotiable.
- Avoid prolonged sitting or inactivity — set reminders to stand and stretch every 30–45 minutes.
- Maintain good posture — practice upright posture consciously, especially while sitting and sleeping.
- Sleep on a firm mattress — soft mattresses can worsen spinal alignment overnight.
- Anti-inflammatory diet — include omega-3 rich foods, vegetables, and reduce processed foods.
- Quit smoking — smoking is strongly associated with worse AS outcomes.
- Regular medical follow-up — stay connected with your doctor and therapist consistently.
Frequently Asked Questions
Yes, AS has a strong genetic component linked to the HLA-B27 gene. However, having a parent with AS does not guarantee you will develop it. Being HLA-B27 positive without any symptoms is also entirely possible and common.
Currently, there is no cure for Ankylosing Spondylitis. However, with the right combination of physiotherapy, exercise, medication, and lifestyle management, the disease can be very effectively controlled. Most patients live normal, active lives.
AS most commonly affects young men between the ages of 17 and 45, though it can occur in women and older individuals. Early diagnosis is critical for the best outcomes, which is why recognizing the symptoms early is so important.
Regular mechanical back pain typically worsens with activity and improves with rest. Ankylosing Spondylitis is the opposite — it improves with movement and worsens after prolonged rest or inactivity. Morning stiffness lasting more than 30 minutes is a key distinguishing feature.